MIS Neck preservation and Short Stem Primary Hip Replacement
As a pupil of Prof . Pipino, his master since 2009, and the ideator ad developer of neck preservation technique, Dr. Zanasi set the MIS approach for this technique .
Preservation of the femoral neck in hip arthroplasty creates a particular biomechanical situation which is clearly different from what is found even after partial neck removal. The femoral neck consists in fact of a "cylinder of cortical bone" that can be used as the "base" for anchoring the stem to the femur, in contrast to the press-fit procedure or other solutions. The mechanical and biological advantages are as follows:
- Primary triplanar stem stability, in particular rotational stability. Rotational movements of the stem are blocked by the tough lateral cortical cylinder of the neck. Resistance to varus-valgus stress and collapse is also increased vertically and frontally.
- Proximal cortical fixation. Primary fixation of the stem is provided by the neck cortex, whereas its mid-distal part is merely held by the metaphyseal cancellous bone and the tip is undersized with respect to the medullary canal.
- Stress loads distributed along physiological lines of stress. Retention of the neck permits preservation of the trabecular systems, along which the stress is distributed towards the diaphysis and the greater trochanter.
- Elasticity of the bone-prosthesis system. Most of the stem is contained within the metaphyseal cancellous bone that lies between the prosthesis and the cortical bone, creating a bone-prosthesis module with variable and integrated elasticity.
- Preservation of the bone-stock. The amount of residual bone following implant of the prosthesis increases, not only because of the presence of the femoral neck, but also as a result of the preservation of most of the metaphyseal cancellous bone. There is therefore greater bone-ingrowth, which is also favoured by the fewer changes in the endosteal blood supply.
- Prosthesis revision is simpler, since the stem can easily be removed and a second neck resection performed. Our clinical and experimental studies confirm that the femoral neck is present for a long time after implant. Finally, we report a study of 200 prostheses with an average follow-up of 10 years, demonstrating neck reabsorption in only 1% of the cases.
The concept of femoral neck preservation during THA was originally proposed several decades ago and continues to divide orthopaedic opinion. The recent trend for bone-conserving surgery has seen a proliferation of cementless short-stem implants enter the market. The questions that therefore arise are: (1) what are the advantages of preserving the femoral neck during THA? and (2) what are the clinical and radiological outcomes of femoral neck-preserving implants? The current literature suggests that there is a biomechanical advantage to retaining the femoral neck. Neck preservation enhances the stability of the femoral prosthesis by reducing interfacial micro-motion and offering greater rotational strength and stiffness, and better resistance to varus-valgus stress. Furthermore, the implantation of a neck-preserving stem has been shown to generate less contact stress on the medial cortex, than a neck resecting implant. Finally, migration studies have reported that preserving the femoral neck reduces distal migration of the femoral stem. The other significant benefit of retaining the femoral neck is greater preservation of native bone stock. Given the increasing number of young patients undergoing THA, the use of a neck-preserving short-stem implant conserves native bone and allows revision to a standard prosthesis at a future date.
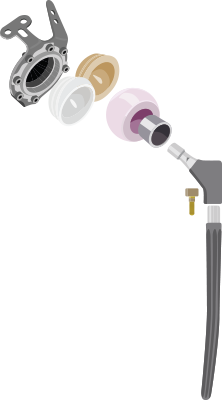
image 1,1bis, 2,3
Bone-saving hip arthroplasty using metaphyseal stems is gaining importance because the number of young patients is on the increase and hip resurfacing is not always indicated. The individual decision for use of a particular type of implant remains crucial because a stem for all indications does not exist. Every patient requires thorough pre-operative planning: short metaphyseal stems attempt to bridge the gap between straight stem implant design and hip resurfacing. A modern femoral implant should spare healthy femoral bone during implantation, loads the neck and metaphysis in a near physiological way; the use of 3-point fixation gives construct a biomechanically favourable offset without unduly lengthening the leg and favours less invasive soft tissue handling during implantation. Short stem aims to remove/reduce thigh pain, “stress shielding”, fracture stem positioning/impacting possibility and to make easier the correct stem positioning (no varus)
Aims of short stem are OPTIMIZATION OF THE ANATOMY( proximal loading with forces trasmitted to calcar region and lateral femoral cortex), TISSUE SPARING, bone preservation. Curved design allows: trochanter major & abductors muscles insertion sparing, high cervical osteotomy level, distal femoral medullar sparing, soft tissues respect, totally respects trochanter major and all abductors muscles. These stems are Compatible with all MIS approaches. Short stem pitfalls are difficult surgical technique, femoral fracturing, undersizing, legh lenght discrepancy.
Standard Revision Hip Arthroplasty
AIMS IN REVISION HIP ARTHROPLASTY (Wolff J. 1986) are:
Complexes Customised Revision Hip Arthroplasty
Not only one fourth of hip and knee revisions of arthroplasties implant are re-revisions following to a suboptimal fixation and suboptimal biomechanical reconstruction of the jointwhen combining standard components, but also hip/knee re-revisions are 3 times more likely to fail compared i.e. to a primary acetabular revisionas we check in clinical practice and literature data every day.
Since 2014 Dr. Zanasi uses patient’s medical scans to design an accurate preoperative 3D plan, including a detailed outline of the procedure, as well, in particular in hip re-revision, as an overview of the screw positioning and lengths. Having such a patient-specific 3D-planned manual of the procedure, our surgical team is able to optimize fixation and minimize the risk of dislocation. That is doable by planning the position of the center of rotation, inclination and anteversion angles preoperatively, reducing intraoperative decisions, and give the patientsa tangible positive impact on their daily life in terms of mobility and pain after receiving a personalized hip implant. For all of them this even mean finally getting out of a wheelchair again.
Furthermore, the application of 3D-printed, patient-specific implants that have been augmented with autologous mesenchymal stem cells (isolated or combined BMSCs and ADSCs), offers a significant opportunity for orthopaedic practice, bone tissue engineering, and regenerative surgery: 3D-printed implants with MSCs seeded on to the implant surface are ideal solution to restore the anatomy and improve the skeletal biology by completing and hastening the healing process.
In our clinical practice, in particular in hip re-revision cases, that most patient cases are Paprosky IIIA and IIIB types, however, the advantageous customized acetabular system has been used in type II, dysplastic and tumor cases as well. It is considered as revision surgeries as well as primary surgeries. Naturally, as the implant is 3D printed and custom-made for each patient, it is not necessary limited to severe cases. It can fit any special defect in which traditional systems do not find out a perfect solution. The main indications are: non-inflammatory degenerative joint disease including osteoarthritis and avascular necrosis, posttraumatic and rheumatoid arthritis, correction of functional deformity, revision procedures where other treatments or devices have failed, treatment in conjunction with tumor resection where bone stock is of poor quality or is inadequate for other reconstructive techniques i.e. as indicated by deficiencies of the acetabulum.
Although a standard solution may be the best one for a standard case, a patient-specific implant is often better suited for more challenging defects. With a Promade solution we get an implant which is pre-operatively designed to match the patient, and optimized for stability and biomechanical performance. Compared to standard implants, whose multiple components need to be pieced intra-operatively, under stress and time pressure, thus jeopardizing the performance, our one-piece solution eliminates the entire process of selection and assembly, and the risks of inter-component moves altogether.
fig6-16